
Darryl's List of Meds
CLICK IMAGE TO GET ALL PILLS LIST
This is a more focused combo, often used for managing hypertension, high lipids, and prostate issues (BPH) with possible ED support. Key Interactions in This Specific ComboOverall, this group has no major life-threatening interactions like serotonin syndrome (from your earlier questions) or severe rhabdomyolysis (e.g., no statins here). However, there are some moderate risks mainly around additive blood pressure lowering (hypotension), which can cause dizziness, lightheadedness, fainting, or falls—especially when standing up quickly.
Practical Tips
This this combo is commonly prescribed together for men with hypertension, high triglycerides, and BPH ± ED, and many tolerate it well. But interactions can vary by dose, age, kidney function, etc. Definitely review this exact list with your doctor or pharmacist—they can check your specific doses, run a full interaction tool, and adjust if needed (e.g., lower tadalafil dose or monitor closer).
also also called Raynaud's phenomenon or Raynaud's disease) is a condition where small blood vessels (usually in the fingers and toes, sometimes nose, ears, or lips) overreact to cold temperatures or emotional stress. This causes temporary spasms (vasospasm), reducing blood flow. The affected areas typically turn white (from lack of blood), then blue (from low oxygen), and finally red (as blood rushes back), often with numbness, tingling, pain, or burning.
There are two main types:
Your blood work helps differentiate these.
Management Tips (Especially Relevant to You)Since you're in Detroit (cold winters!), these can help prevent attacks and fit with your BPH/hypertension meds (tamsulosin, nifedipine, etc.—nifedipine is actually sometimes used off-label for Raynaud's as a vasodilator):
These results are encouraging—no strong red flags for serious autoimmune disease here. Track your symptoms and follow up with your doctor (primary or rheumatologist) for personalized interpretation—they know your full history/age/other labs.
Your nifedipine helps both BP and Raynaud's vessel relaxation—keep using warmth/prevention tips to minimize attacks. If leg symptoms worsen or you get sores/ulcers from Raynaud's (rare in primary), see your doc promptly. Yes, some of the medications you're taking (Gemfibrozil, Lisinopril-HCTZ, Nifedipine, Tadalafil, and Tamsulosin every other day) can contribute to increased stomach acid, heartburn, acid reflux (GERD symptoms), or related digestive issues like indigestion/upset stomach. These effects don't mean the drugs "create" more acid in everyone, but they can irritate the stomach lining, relax the lower esophageal sphincter (the muscle that keeps acid in the stomach), cause dyspepsia (indigestion), or worsen existing reflux. Here's a breakdown based on reliable sources like Mayo Clinic, Drugs.com, MedlinePlus, and others:
Overall:
If you describe your specific symptoms (e.g., burning in chest, sour taste, timing after doses), I can help narrow it down more! |
|
Here are the key interactions between Losartan Potassium (an ARB used for high blood pressure, kidney protection in diabetes, etc.) and your current medications: Gemfibrozil, Lisinopril-HCTZ, Tadalafil, and Tamsulosin (taken every other day). This is based on standard drug interaction data from reliable sources like Drugs.com, Mayo Clinic, and clinical guidelines. Losartan is generally well-tolerated, but interactions can increase risks like low blood pressure (hypotension), high potassium (hyperkalemia), or kidney issues—especially relevant with your hypertension and prostate management.
Overall Summary for Your Combo
|
| Claim ID | Claim Type | Member Name | Paid Date | Provider Name | Claim Status |
Total Billed Amount |
Total Paid |
| 24089E0134610 | Professional | DATE, DARRYL R | 4/4/2024 | JADDOU, NEIL D | PAID | $150.00 | $78.66 |
| 24285E0087649 | Professional | DATE, DARRYL R | 10/17/2024 | JADDOU, NEIL D | PAID | $240.00 | $124.41 |
| 25269Z0049954 | Professional | DATE, DARRYL R | 9/30/2025 | JADDOU, NEIL D | PAID | $375.00 | $122.76 |
| 25275Z0070790 | Professional | DATE, DARRYL R | 10/7/2025 | JADDOU, NEIL D | PAID | $375.00 | $122.76 |
| 25323Z0010457 | Professional | DATE, DARRYL R | 11/24/2025 | JADDOU, NEIL D | PAID | $250.00 | $98.23 |
| 25325Z0099333 | Professional | DATE, DARRYL R | 11/25/2025 | TOOLEY, TREVOR R | PAID | $336.00 | $71.78 |
| 25328Z0047203 | Professional | DATE, DARRYL R | 11/26/2025 | JADDOU, NEIL D | PAID | $350.00 | $90.80 |
| 25336Z0059982 | Professional | DATE, DARRYL R | 12/4/2025 | JADDOU, NEIL D | PAID | $200.00 | $88.64 |
| 25340Z0044481 | Professional | DATE, DARRYL R | 12/9/2025 | JADDOU, NEIL D | PAID | $240.00 | $124.41 |
| 25342Z0010799 | Institutional | DATE, DARRYL R | 12/11/2025 | COREWELL HEALTH WILLIAM BEAUMONT UN | PAID | $5,686.01 | $595.84 |
| 25345Z0059626 | Professional | DATE, DARRYL R | 12/15/2025 | FRANCOIS, HOWARD | PAID | $80.00 | $10.66 |
| 25343Z0092901 | Professional | DATE, DARRYL R | 12/15/2025 | HUSAIN, SYED A | PAID | $285.00 | $107.57 |
| 25345Z0081226 | Professional | DATE, DARRYL R | 12/15/2025 | SHANLEY, CHARLES J | PAID | $475.00 | $23.86 |
| 25347Z0035919 | Professional | DATE, DARRYL R | 12/18/2025 | PETTENGILL, PATRICK T | PAID | $276.00 | $77.24 |
| 25347Z0064941 | Professional | DATE, DARRYL R | 12/18/2025 | TEHRANISA, JASON S | PAID | $1,654.00 | $77.24 |
| 25351Z0022817 | Institutional | DATE, DARRYL R | 12/22/2025 | UNIVERSITY OF MICHIGAN | PAID | $5,545.00 | $341.17 |
| 25354Z0048583 | Professional | DATE, DARRYL R | 12/26/2025 | JADDOU, NEIL D | PAID | $150.00 | $78.28 |
| 26009Z0063031 | Professional | DATE, DARRYL R | 1/13/2026 | JADDOU, NEIL D | PAID | $175.00 | $110.16 |
| 26024Z0061932 | Professional | DATE, DARRYL R | 1/29/2026 | JADDOU, NEIL D | PAID | $150.00 | $78.28 |
| 26051Z0058635 | Professional | DATE, DARRYL R | HUSAIN, SYED A | PAY | $185.00 | $82.43 | |
| TOTALS | $17,177.01 | $2,505.18 |
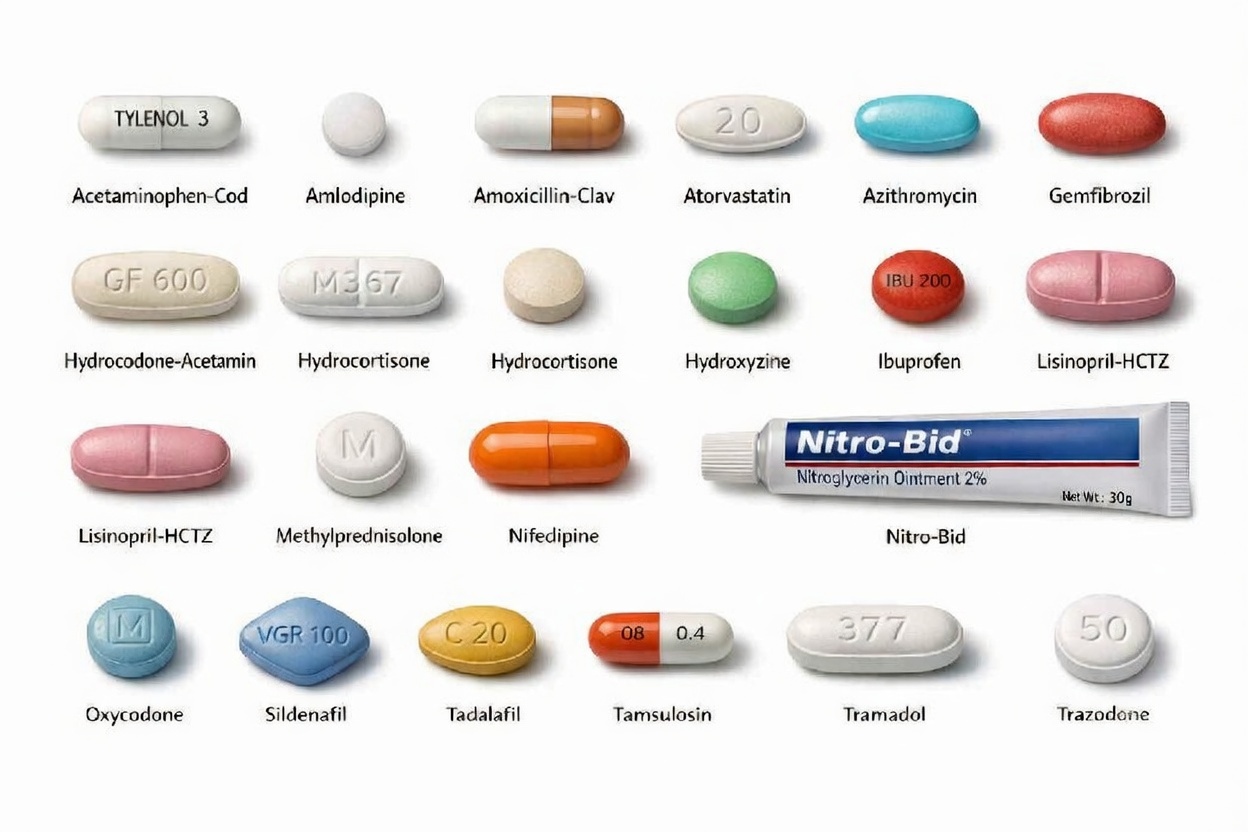
| Pill and info Dosage size of each pill |
| Acetaminophen-cod #3 Tablet Amlodipine Besylate 10 Mg Tab Amoxicillin-clav 875-125mg Tab Atorvastatin 10 Mg Tablet Azithromycin 250 Mg Tablet Gemfibrozil 600 Mg Tablet Hydrocodone-acetamin 5-325 Mg Hydrocortisone 2.5% Cream Hydroxyzine Hcl 50 Mg Tablet Ibuprofen 600 Mg Tablet Lisinopril-hctz 20-12.5 Mg Tab Losartan Potassium 25 Mg Tab Methylprednisolone 4 Mg Dosepk Nitro-bid 2% Ointment Oxycodone Hcl (Ir) 5 Mg Tablet Sildenafil 20 Mg Tablet Sildenafil 50 Mg Tablet Tadalafil 5 Mg Tablet Tamsulosin Hcl 0.4 Mg Capsule Tramadol Hcl 50 Mg Tablet Trazodone 50 Mg Tablet |

